One of the first ideas I had about how to measure local variation in heteronormativity was to look at hate crimes statistics. The logic is that hate crimes are a direct and extreme expression of heteronormativity. The FBI issues a report every year documenting the number of crimes reported as being bias-motivated, and also where they happen and against whom the violence is targeted.
But a strange thing happened when I looked at the data - there were a fair number of bias-motivated crimes reported from San Francisco and New York City, and virtually none from the places I expected to be havens of homophobia. The most likely explanation is that the number of hate crimes reported is a lousy measure of the number of hate crimes committed, and is a better measure of the degree to which a person reporting a hate crime to the police is taken seriously. So, in a way, hate crimes reporting may be a decent measure of heteronormativity, but in the opposite direction of what you'd expect at first: the more hate crimes reported, the friendlier the social environment is for TBLG people.
But, it gets more complicated. There are two ways not to have much conflict between dominant and subordinate groups. One way is for everyone to get along. Another way is for the subordinate group to "mind its manners" and steer clear of offending the sensibilities of the dominant group. So even if the incidence of hate crimes were a good measure of homophobia, it would be complicated because you'd expect the number of crimes to be low in areas where gay people have learned that the best thing to do is stay deeply closeted, or to get out of Dodge. And even though areas that are "gay meccas" allow us to express ourselves more freely, this can incite hardened haters in our midst to violence, like Dan White. "Gay meccas" can also attract hardened haters with violent intentions, and thus one often sees violent hate crimes centered around gay bars and cruising areas.
Anyway, it had been over ten years since I looked at the hate crimes data, and a lot happened since then. So I was curious to see what has changed.

I have to admit, I'm intrigued by data like this. I don't know what story they are telling. I anticipated that with the rapid change in societal attitudes about homosexuality, we'd see a steady growth in the number of reported anti-gay hate crimes. But, as you can see in the graph below, the number of reported anti-gay hate crimes rose pretty steadily until 2001, and has pretty much leveled off since then.

So maybe that's a good sign - of increasing tolerance, acceptance, and even celebration breaking out in some corners of the country. But it could mean a lot of things, and when you dig down into where these anti-BLG crimes are being reported from, it's still predominantly from the gay meccas - large coastal cities and also university towns all across the country. I suspect that there are lots of anti-gay crimes not being reported at all, especially in rural areas and the South.
Maybe the peak in 2001 highlights a shift in the attention of bigots, towards a new bogeyman. There's certainly plenty of evidence that anti-Arab (much of the darker orange slice in the graph below), and anti-Muslim (the bright green slice in the next graph down) spiked hard in 2001, and there has been a sustained increase in anti-Islamic crimes since then compared to the 1990's. But I think the idea of bigots turning away from the gays and towards the Muslims is at best a partial story. Also of interest to note in the graph below is that the number of anti-Black crimes reported by the FBI was definitely lower in the first two years of the Obama administration. Evidence of a post-racial America? I strongly doubt it - although the post-racial narrative might explain it if one considers that some of the more "post-racist" (emphasis on racist) police may be harder to convince that a bias-motivated crime has occurred, and thus less likely to report it as such. It would certainly be interesting to look at those trends in the wake of the 2010 retrenchment election.


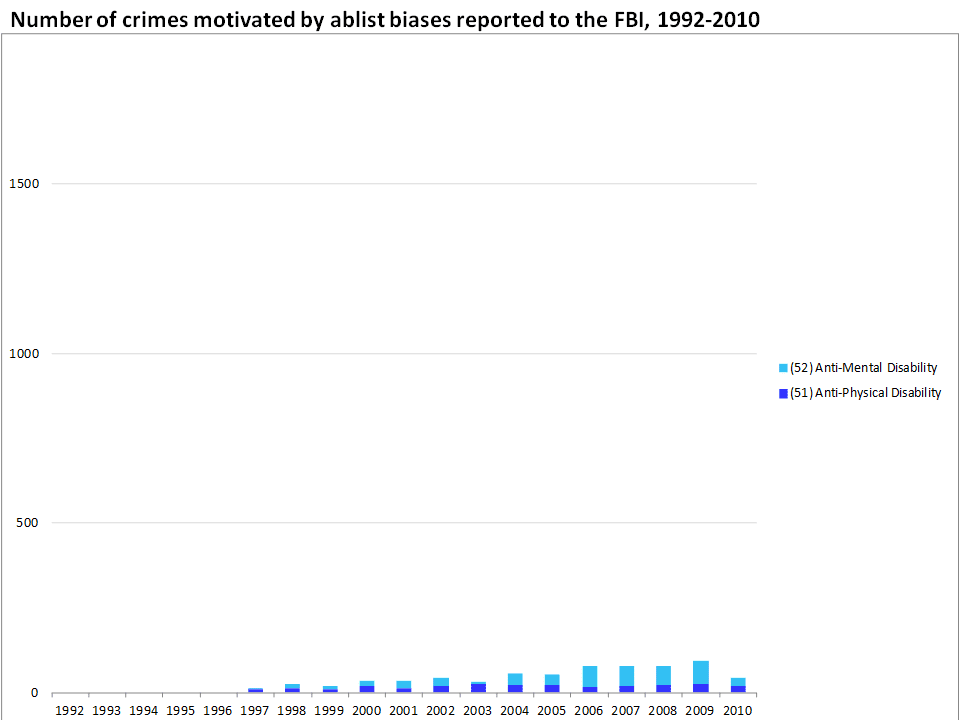
Another interesting twist to the tospy-turvy world of hate crimes reporting is the biases for which no reporting category is even available. There were no crimes reported as being motivated by ablism before 1997. It's not that a glorious heyday of equanimity passed in 1996, but rather that there was simply no category available even to describe these bias motivations in the FBI's system. Even today (or at least up to 2010), the number of crimes reported as being directed by ablist biases numbers in the dozens per year, across the entire country. So here's another example indicating that the nature of the bias itself prevents it from being recognized and recorded.
So, that seems like a pretty exhaustive list: crimes motivated by bias on the basis of race, ethnicity, religious preference, sexual orientation, and ability. Or does it? Notice that there's simply no category to record crimes motivated by bias against transgender people yet, or intersex, or even bias against women. I wouldn't be surprised if the number of reported hate crimes would double if rapes motivated by misogyny were reported as such.
Also, in a nation where most sources of intolerance are weakening, intolerance against fat people is on the rise. Plug for a great article on anti-fat bias and media portrayals of disembodied depersonalized fatness.
Also, in a nation where most sources of intolerance are weakening, intolerance against fat people is on the rise. Plug for a great article on anti-fat bias and media portrayals of disembodied depersonalized fatness.
 I have to admit, I'm pretty ambivalent about organizing around hate crimes as a means to end prejudice. It's not for lack of trying. As my time with ActUp/RI wound down, I turned to advocacy around hate crimes - even made myself into a bit of a spokesmodel in the wake of being beaten about the head on Thayer Street in Providence (that's me standing and gesturing to another victim in that attack). I got involved in training a few police departments in Rhode Island, but I found that re-hashing my story as a hate crime "victim" was a source of re-victimization, and left me feeling dis-empowered and alienated, especially after some of the more intense police training sessions.
I have to admit, I'm pretty ambivalent about organizing around hate crimes as a means to end prejudice. It's not for lack of trying. As my time with ActUp/RI wound down, I turned to advocacy around hate crimes - even made myself into a bit of a spokesmodel in the wake of being beaten about the head on Thayer Street in Providence (that's me standing and gesturing to another victim in that attack). I got involved in training a few police departments in Rhode Island, but I found that re-hashing my story as a hate crime "victim" was a source of re-victimization, and left me feeling dis-empowered and alienated, especially after some of the more intense police training sessions.





